

Even asking how best to wean drug abusers off opioids can raise hackles. Addiction specialists have straddled a philosophical divide over the use of pharmaceuticals in the process. But the side advocating against medication assisted treatment is shrinking in Tennessee and nationwide.
One line of thinking is that freedom from all drugs is the only real recovery. So it’s been difficult for those with that mindset to embrace special opioids that tame the cravings and ward off the misery of withdrawal sickness.
“Actually, it’s in my pocket,” says Chris Dummer, a manager at a Nashville deli, pulling out a container on his keyring that holds his daily dose. He dissolves one small pill under his tongue each morning. “There’s a lot of power in that tiny package.”
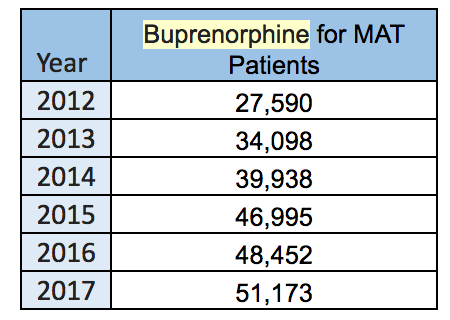
It’s often known better by brand names like Suboxone. Buprenorphine is the generic term, and it has quickly become one of the biggest-selling drugs in the U.S. In Tennessee, prescriptions have doubled in the last five years.
For Dummer, an amateur photogapher with a degree from MTSU, the medication has helped keep him staty sober for six years, though he plans to wean himself completely soon. It’s a real success story.
And yet, he’s hesitant to discuss it openly because among the 12-step community, like Narcotics Anonymous, it’s still taboo.
“I know a lot of people don’t tell anybody that they’re taking it, for fear of some kind of retribution or just being looked down upon in general,” he says. “There are a lot of people who say that you do get high off the drug and it’s just replacing one drug for another.”
It is replacing one opioid with another (
explained here). But buprenorphine is much harder to abuse because it has a ceiling effect and in most formulations is combined with an overdose reversal agent. That means taking a handful of them won’t get someone any higher and shouldn’t kill them, though
some overdose deaths in Tennessee have been blamed on the drug.
Still, buprenorphine has a dark side that has kept medical professionals like counselor Michael Reynolds from recommending the treatment.
“I guess my biggest fear is diversion,” says Reynolds, a program manager for Centerstone, which works with drug courts in Tennessee.
The pills are often
sold on the street. It’s counterintuitive, but if addicts can’t get their opioid of choice, buprenorphine will at least keep the sickness of withdrawal from coming on. So because of the street value, this drug for treating opioid abuse could be sold to help finance the addiction itself.
More:
Why Are So Many Suboxone Patients Buying The Drug On The Streets?
Reynolds says Centerstone in Tennessee has had a hard rule against prescribing patients buprenorphine until now. He’s had a reluctant conversion, as overdose deaths weigh on his conscience.
“How many people are we trying to save here? How many do we let die?” he asks. “Even me, I’d say yeah, I had a change of heart and have kinda come around, that every life is worth saving.”
This summer, Centerstone will start offering medication assisted treatment like buprenorphine and another monthly injectable form with the brandname Vivitrol. Reynolds says federal authorities are requiring it to qualify for grants.
But Centerstone is not the only institution known for preaching abstinence that’s coming around as the opioid epidemic becomes more deadly. So is Nashville-based American Addiction Centers — one of the largest rehab companies in the country.
“We’ve had this dialogue going on within the past 12 months or so,” medical director Mark Calarco says. “We’ve really ramped it up now where we have active programs at every facility.”
Calarco says it’s gotten to a point that programs which expect abstinence are viewed as offering substandard care.
Opening Access Wider
And the big believers in buprenorphine are pushing for even more access. Becoming a prescriber takes a special license, and given
the rate of overdoses in the state, Tennessee doesn’t have nearly as many licensed physicians as it needs.
Tennessee also still doesn’t allow nurse practitioners and physician assistants to prescribe buprenorphine. There was legislation that would have brought Tennessee in line with almost every other state, but it was amended to only study the issue.
“It’s incredibly hard to find physicians of any stripe who have the experience with addiction medicine and the DEA waiver to be able to prescribe the buprenorphine in order to make this work,” says Brian Haile, CEO of Neighborhood Health, which now requires all of its newly-hired doctors to get a buprenorphine license and continues to push for NPs and PAs to have privileges in the state.
Buprenorphine For Life?
So the debate is moving from whether to use buprenorphine to how long. And that’s a tough question because getting off the drug can be just as hard as kicking pain pills or heroin.
In a house-turned-buprenorphine clinic in Berry Hill, Dr. Richard Soper invites a patient back for a brief counseling session before writing her monthly prescription. He accepts that this may lead to life-long dependence for many.

But like many buprenorphine fans, he points to other medications for chronic disorders. Yes, it’s possible to get off of them, but Soper says physicians would never insist.
“We don’t do that for high blood pressure, we don’t do that for asthma, we don’t do that for diabetes. We don’t do that for any chronic medical disorder,” he argues.
For Mary Gilliam, who drives an hour from Shelbyville to see Soper each month, she has given up on ever getting off buprenorphine.
“I don’t even pretend,” she says. “I’m so over that.”
Gilliam is a former nurse, a mother of two, who says she got hooked on Lortab after a running injury and eventually ended up shooting heroin.
She says it’s not a miracle drug. She’s relapsed more times than she can count, and expects heroin will continue to derail her from time to time. But Gilliam says buprenorphine makes it possible to get back on track.
“I’ve been through so many [abstinence based] treatment centers, and it’s such a — I hate to use the word joke — but futile,” she says. “As far as I can tell, you’re going to have to replace that medicine with this medicine. Period. I don’t know any other way around it.”
